Pythium keratitis: clinical course of an emerging scourge
Abstract
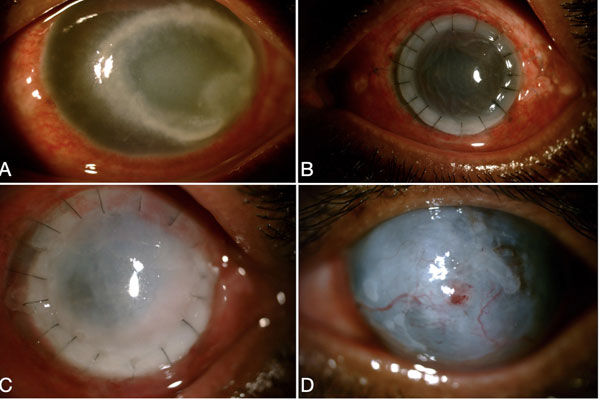
We hereby report two cases of the emerging and devastating Pythium keratitis for their different presentations, prolonged clinical course, and suspicion of recurrence after therapeutic penetrating keratoplasty (TPK). The history, clinical presentation, investigations including smears, cultures, polymerase chain reaction (PCR) and confocal microscopy, the tumultuous course of the infection, and outcome of TPK have been discussed for two cases having this unusual and severe emerging infection. These two cases demonstrate that Pythium keratitis can present as a central reticular or peripheral guttering corneal ulcer with dense infiltration. PCR is a valuable tool for diagnosis. Pythium keratitis has a severe and prolonged clinical course. Response to antibiotics is modest and needs to be closely monitored. It can present with inflammation after TPK that mimics the dreaded recurrence of the infection. Pythium keratitis presents variably and can be suspected from typical clinical and microbiological findings. It needs protracted treatment with close follow-up. Although the infection is known to
recur in the therapeutic graft, not all recurrences are what they seem.
References
He H, Liu H, Chen X, Wu J, He M, Zhong X. Diagnosis and Treatment of Pythium Insidiosum Corneal Ulcer in a Chinese Child: A Case Report and Literature Review. Am J Case Rep. 2016;17:982–988.
Agarwal S, Iyer G, Srinivasan B, et al. Clinical profile of pythium keratitis: perioperative measures to reduce risk of recurrence. Br J Ophthalmol. 2018;102(2):153–157.
Agarwal S, Iyer G, Srinivasan B, et al. Clinical profile, risk factors and outcome of medical, surgical and adjunct interventions in patients with Pythium insidiosum keratitis. Br J Ophthalmol. 2019;103(3):296–300.
Hasika R, Lalitha P, Radhakrishnan N, et al. Pythium keratitis in South India: Incidence, clinical profile, management, and treatment recommendation. Indian J Ophthalmol 2019;67(1):42-47.
Krajaejun T, Sathapatayavongs B, Pracharktam R, et al. Clinical and epidemiological analyses of human pythiosis in Thailand. Clin Infect Dis. 2006;43(5):569–576.
Sharma S, Balne PK, Motukupally SR, et al. Pythium insidiosum keratitis: clinical profile and role of DNA sequencing and zoospore formation in diagnosis. Cornea. 2015;34(4):438–442.
Bagga B, Sharma S, Madhuri Guda SJ, et al. Leap forward in the treatment of Pythium insidiosum keratitis. Br J Ophthalmol. 2018;102(12):1629–1633.
Copyright (c) 2020 Radhika Natarajan, Ankit Anil Harwani, Ramya Ravindran

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors who publish with this journal agree to the following terms:
- Authors retain copyright and grant the journal right of first publication, with the work twelve (12) months after publication simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal.
- Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the journal's published version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgement of its initial publication in this journal.
- Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See The Effect of Open Access).