Microsporidial stromal keratitis: an uncommon etiology of bilateral simultaneous corneal infection
Abstract
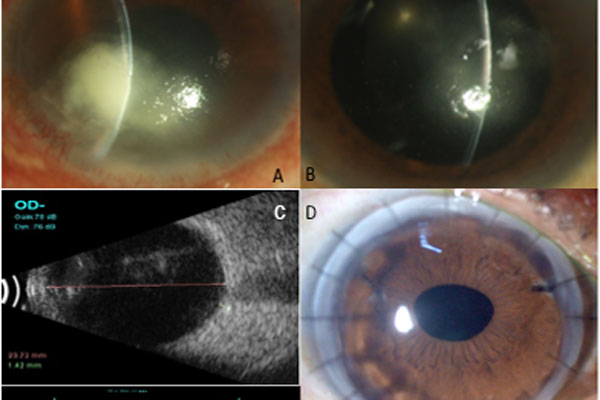
We report three cases of bilateral microsporidial keratitis, which is an unusual presentation. All three patients presented with bilateral, simultaneous, asymmetrical, deep stromal corneal infiltrates with symptoms ranging from 5 to 12 months. Predisposing factors were noted in two of three patients. Corneal scrapings for microbiology and histopathology of corneal tissue revealed microsporidial spores from both eyes of all patients. There was no response to medical therapy and all underwent bilateral corneal transplantation. Case one additionally had recurrences in the graft and underwent repeat keratoplasties and eventually keratoprosthesis. Microsporidial stromal keratitis is a possible cause of keratitis in cases of very long-standing, indolent, culture-negative, deep stromal corneal infiltrates. So far, this infection has been reported as unilateral; however, we report these cases of bilateral infection, which is rare. Corneal transplantation is the preferred line of management due to lack of response to medical therapy.
References
Metcalfe TW, Doran RM, Rowlands PL, Currey A, Lacey CJ. Microsporidial keratoconjunctivitis in a patient with AIDS. Br J Ophthalmol. 1992; 76:177–178.
Sabhapandit S, Murthy SI, Garg P, Korwar V, Vemuganti GK, Sharma S. Microsporidial Stromal Keratitis: Clinical Features, Unique Diagnostic Criteria, and Treatment Outcomes in a Large Case Series. Cornea. 2016;35(12):1569-1574
Yoken J, Forbes B, Maguire AM, Prenner JL, Carpentieri D. Microsporidial endophthalmitis in a patient with acute myelogenous leukemia. Retina. 2002;22(1):123-125.
On Annie LH, Ray M. Bilateral simultaneous infective keratitis. Cont Lens Anterior Eye. 2017;40(4):224-227.
Tzamalis A, Romano V, Cheeseman R, Vinciguerra R, Batterbury M, Willoughby C. Bandage contact lens and topical steroids are risk factors for the development of microbial keratitis after epithelium-off CXL. BMJ Open Ophthalmol. 2019;16;4(1)
Vemuganti GK, Garg P, Sharma S, Joseph J, Gopinathan U, Singh S. Is microsporidial keratitis an emerging cause of stromal keratitis? A case series study. BMC Ophthalmol. 2005;5:19
Joseph J, Sridhar MS, Murthy S, Sharma S. Clinical and microbiological profile of microsporidial keratoconjunctivitis in southern India. Ophthalmology. 2006;113:531–537.
Sood AB, Debiec MR, Yeh S, Grossniklaus HE, Randleman JB. Microsporidial stromal keratitis and endophthalmitis in an immunocompetent patient. J Ophthalmic Inflamm Infect. 2016;6(1):30
Mathis A, Weber R, Deplazes P. Zoonotic potential of the microsporidia. Clin Microbiol Rev. 2005;18(3):423-45
Coca M, Kim J, Shenoy S, Chévez-Barrios P, Kapur M. Microsporidial Stromal Keratitis: Successful Treatment with Topical Voriconazole and Oral Itraconazole. Cureus. 2016 20;8(12):934.
Copyright (c) 2020 Pragnya R. Donthineni, Dr., Somasheila I. Murthy, Joveeta Joseph, Prashant Garg, Manisha Acharya, Virender Sangwan

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors who publish with this journal agree to the following terms:
- Authors retain copyright and grant the journal right of first publication, with the work twelve (12) months after publication simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal.
- Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the journal's published version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgement of its initial publication in this journal.
- Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See The Effect of Open Access).