Macular buckle with Morin–Devin T implant for pathological myopia with macular hole
Abstract
Introduction: Pathological myopia is commonly associated with myopic traction maculopathy, which includes foveoschisis, foveal retinal detachment, macular hole (MH) and/or macular detachment (MD). Macular buckling is a rarely practiced extraocular surgical modality these days. The purpose of this study was to investigate the efficacy of primary buckling with Morin–Devin T implant for MD with MH and posterior staphyloma.
Case description: A 52-year-old female presented with light perception vision in her right eye with posterior staphyloma, localized neurosensory detachment, and MH. She underwent primary macular buckling with Morin–Devin T implant. During the immediate postoperative day the wedge indentation was found misaligned to the fovea. A revision surgery was done after 2 weeks for repositioning of the macular wedge. Spectral domain optical coherence tomography confirmed indentation at the MH with resolution of subretinal fluid and hole closure. Her BCVA was 2/60 at 3 months postoperative and it remained the same even at 6 months of follow-up.
Conclusions: Primary macular buckling can be an effective procedure in eyes with MH with detachment and posterior staphyloma with or without associated foveoschisis. Morin–Devin T implant placement is a relatively simple procedure with short surgical time and excellent outcome.
References
Wong YL, Saw SM. Epidemiology of pathologic myopia in Asia and worldwide. Asia Pac J Ophthalmol. 2016;5(6):394-402.
Johnson MW. Myopic traction maculopathy: pathogenic mechanisms and surgical treatment. Retina. 2012;32(Suppl 2):205-210.
Gaucher D, Haouchine B, Tadayoni R, et al. Long-term follow-up of high myopic foveoschisis: natural course and surgical outcome. Am J Ophthalmol. 2007;143:455-462.
Shimada N, Ohno-Matsui K, Baba T, Futagami S, Tokoro T, Mochizuki M. Natural course of macular retinoschisis in highly myopic eyes without macular hole or retinal detachment. Am J Ophthalmol. 2006;142:497-500.
Ikuno Y, Sayanagi K, Oshima T, et al. Optical coherence tomographic findings in macular holes and retinal detachment after vitrectomy in highly myopic eyes. Am J Ophthalmol. 2003;136:477-481.
Mateo C, Burés-Jelstrup A, Navarro R, Corcóstegui B. Macular buckling for eyes with myopic foveoschisis secondary to posterior staphyloma. Retina. 2012;32(6):1121-1128.
Baba T, Tanaka S, Maesawa A, Teramatsu T, Noda Y, Yamamoto S. Scleral buckling with macular plombe for eyes with myopic macular retinoschisis and retinal detachment without macular hole. Am J Ophthalmol. 2006;142:483-487.
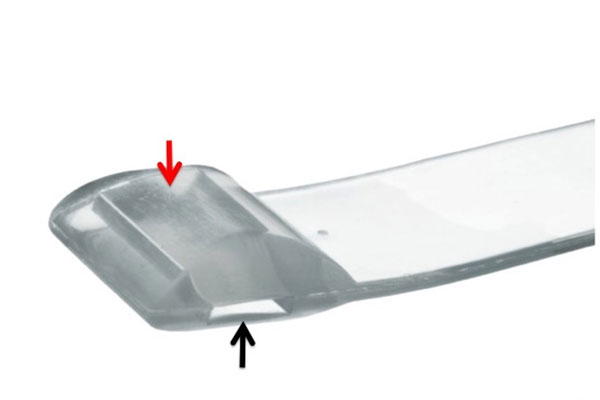
Devin F, Tsui I, Morin B, Duprat JP, Hubschman JP. T-shaped scleral buckle for macular detachments in high myopes. Retina. 2011;31(1):177-180.
Takano M, Kishi S. Foveal retinoschisis and retinal detachment in severely myopic eyes with posterior staphyloma. Am J Ophthalmol. 1999;128:472-476.
Kanda S, Uemura A, Sakamoto Y, Kita H. Vitrectomy with internal limiting membrane peeling for macular retinoschisis and retinal detachment without macular hole in highly myopic eyes. Am J Ophthalmol. 2003;136:177-180.
Shukla D, Dhawan A. Foveoschisis after vitrectomy for myopic macular hole with secondary retinal detachment. Eye. 2009;23:2124-2125.
Ando F, Ohba N, Touura K, Hirose H. Anatomical and visual outcomes after episcleral macular buckling compared with those after pars plana vitrectomy for retinal detachment caused by macular hole in highly myopic eyes. Retina. 2007;27:37-44.
Bedda AM, Hadi AMA, Lolah M, Shafy MSAA. A new sutureless illuminated macular buckle designed for myopic macular hole retinal detachment. J Ophthalmol. 2017;Article ID 6742164:7.
Mateo C, Medeiros MD, Alkabes M, Jelstrup AB, Postorina M, Corcostegui B. Illuminated Ando plombe for optimal positioning in highly myopic eyes with vitreoretinal diseases secondary to posterior staphyloma. JAMA Ophthalmol. 2013;131(10):1359-1362.
Susvar P, Vinay KS. Macular buckle in myopia. Sci J Med Vis Red Foun. 2015;XXXIII:71-74.
Copyright (c) 2020 Abhishek Anand, Lalit Agarwal, Nisha Agrawal, Atul Kumar Anand

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors who publish with this journal agree to the following terms:
- Authors retain copyright and grant the journal right of first publication, with the work twelve (12) months after publication simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal.
- Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the journal's published version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgement of its initial publication in this journal.
- Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See The Effect of Open Access).